
As the COVID-19 pandemic unfolds, the increasing demand and supply of data has spawned a breadth of data visualization tools (DVTs).
Not surprisingly, we are witnessing an outpour of COVID-19 DVTs in India, including the Coronavirus India Dashboard and India COVID-19 tracker, among others. In both nutrition and the COVID-19 response, it is critical that DVTs are designed for their intended impact.
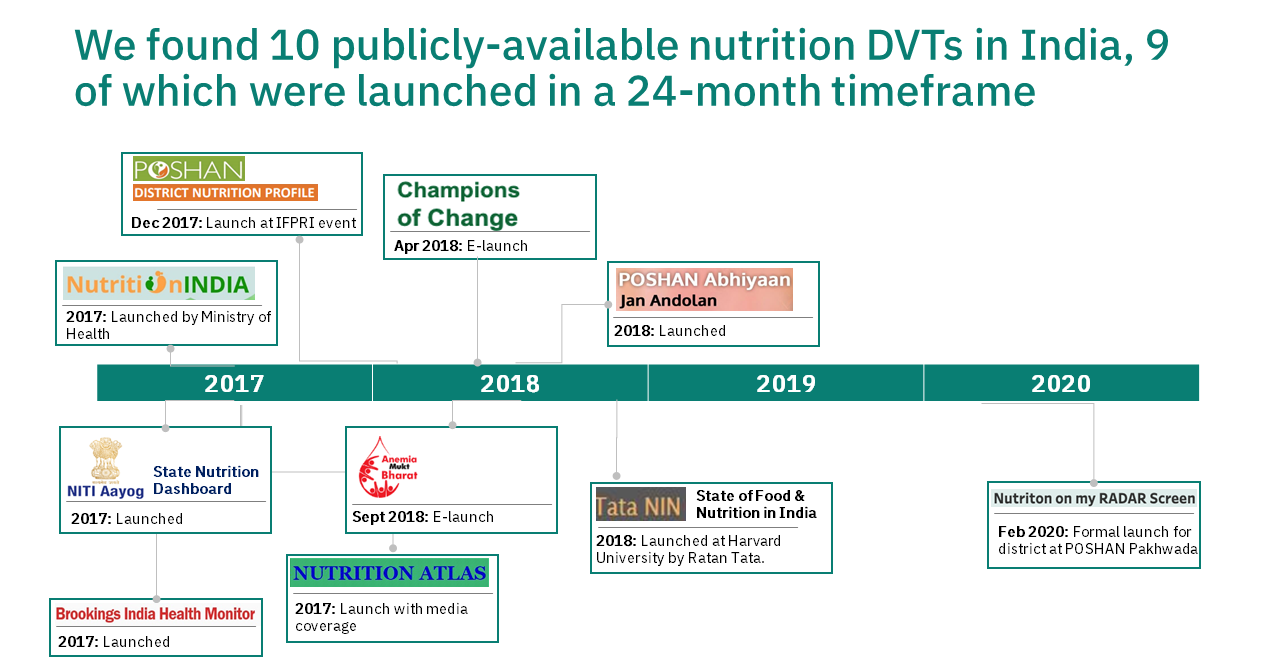
In recent years, India has also seen a surge in DVTs to communicate nutrition data in visual formats. This surge resulted from the launch of the Digital India flagship program that promotes governance through digital platforms, and the need for monitoring progress of POSHAN Abhiyaan, India’s flagship nutrition program [1].
To examine how DVTs contribute to the India nutrition landscape (and to identify best practices), we conducted an analysis of 10 Indian DVTs. These tools included:
1. Aspirational Districts Monitoring Dashboard (Champions of Change)
2. Anemia Mukt Bharat Dashboard (POSHAN Abhiyaan)
3. Jan Andolan Dashboard (POSHAN Abhiyaan)
4. NITI Aayog State Nutrition Dashboard
7. POSHAN District Nutrition Profiles
8. TATA NIN Center for Excellence in Public Health Nutrition
9. The Brookings India Health Monitor
10. Nutrition on my RADAR Screen
Our review revealed the following four insights:
1. Although nutrition DVTs in India have clearly defined purposes and audiences, few have specified how their DVT will contribute to users taking action.
The majority of the reviewed DVTs clearly articulated their purpose around supporting planning, implementation, and monitoring of nutrition programs more broadly or specific sub-topics within nutrition. However, most of these purposes were broadly defined with a wide range of users that included government stakeholders, researchers, and NGOs. Only a few DVTs had clarity on the specific decisions and behaviors that the DVTs were trying to change and how they expected to engage their targeted users. The POSHAN District Nutrition Profiles (DNPs) are a good example of a DVT that presents a clear pathway to achieve its goal to create awareness and facilitate evidence-based decision making at the district level with a targeted set of decision makers (District Panchayati Raj Officers, District Program Officers, Medical Officers, etc.), who are actively engaged and provided regular trainings on DVT use.
2. Overlapping indicators across DVTs result in confusion if there are different definitions and data sources.
In our review, we found that in some cases DVTs reported on the same indicator but used different indicator definitions and data sources. As a result, indicator point estimates visualized can vary across DVTs. This may cause confusion, as illustrated in the example below of how different DVTs communicate “early initiation of breastfeeding” in Araria district of Bihar. The table below shows differences in both indicator definitions as well as data sources used, and corresponding point estimates.
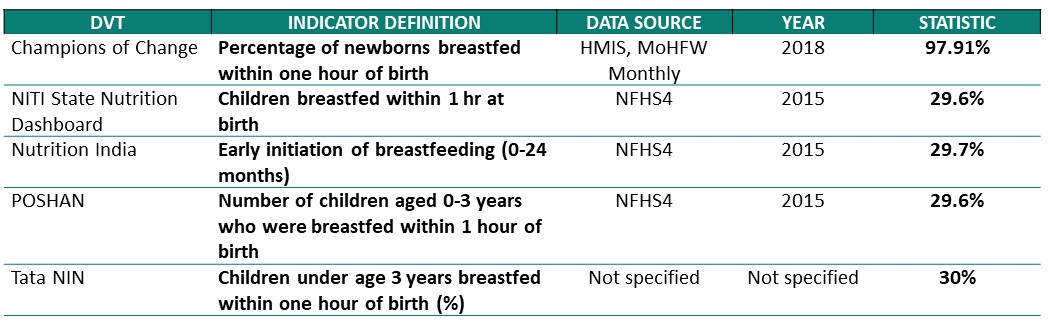
Example of differences in indicator definition and data source: Early initiation of breastfeeding in Araria District, Bihar
3. There is need for more program input and intervention coverage indicators to support action by decision-makers.
While outcome indicators are important for assessing the “state of nutrition,” these indicators alone do not provide a decision-maker the information they need to take action. To improve outcomes, program input indicators (e.g. iron and folic acid tablets supply) and program coverage indicators (e.g. percentage of children who were ever weighed in the last 12 months) are critical to identify what steps can be taken to improve outcomes. Unfortunately, DVTs are reporting on limited number of input indicators. Likewise, DVTs have few coverage indicators especially for programs targeted at adolescents and newborn care. Since several DVTs have identified their goals to support implementation and monitoring, there is a strong need for program input and coverage indicators to be collected and reported.
4. DVTs can take additional steps to improve user interface.
In our review, we found DVT producers are providing support to users via user guides, trainings, and WhatsApp groups. However, this support might have been better geared if producers had connected with targeted users ahead of DVT development to both understand user needs and data literacy; we only found two DVTs that did some type of user engagement. In addition, DVTs can further improve their users ability to interpret data by ensuring labels are used for visualizations (see Example 1) and that a reference value [2] is provided to determine whether a point estimate is on target or off target (see Example 2).
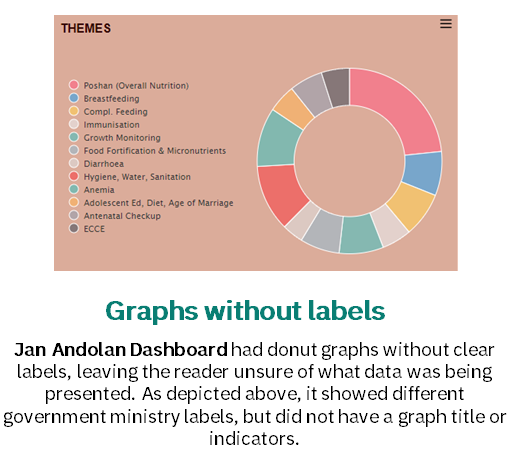
Example 1. Graphs without labels
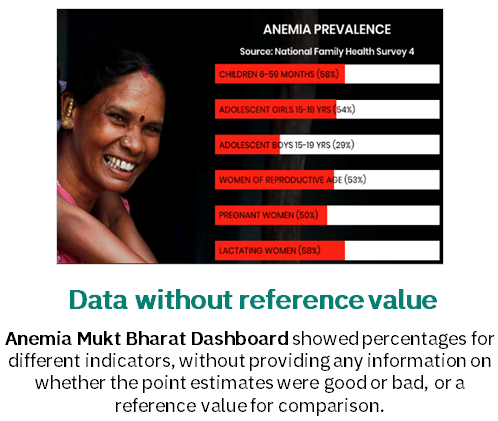
Example 2. Point estimates without reference value
COVID-19 has led to an outpour of COVID-19 DVTs in India (and globally) that have mixed success with conveying clear action/audience. Seeing the landscape of COVID-19 DVTs, it seems they confront similar issues– non-strategic indicator choices/definitions, lack of ties to action, etc. We expect that our findings will be helpful for producers of DVTs, in nutrition and for the COVID-19 pandemic, so that these tools are set up effectively to facilitate users to access, interpret and use data for decision-making.
Full findings from the India DVT landscaping are available here. To learn more about the global landscaping conducted by R4D, please find details here.
[1] The Prime Minister’s Overarching Scheme for Holistic Nutrition (POSHAN) Abhiyaan or National Nutrition Mission, is Government of India’s flagship program to improve nutritional outcomes for children, pregnant women and lactating mothers. Launched by the Prime Minister on International Women’s Day on 8 March 2018, from Jhunjhunu in Rajasthan, POSHAN Abhiyaan directs the attention of the country towards the problem of malnutrition and addresses it in a mission-mode.
[2] A reference value provides the reader with a point of reference on whether the presented statistic is good or bad. For example, a reference value could be a national target, or international cut offs for mild, moderate, and severe anemia.