
Infant and young child feeding (IYCF) counselling is important to facilitate optimal feeding practices and improve child survival. I sat down with Sunny Kim, Research Fellow with the International Food Policy Research Institute and DataDENT team member, to discuss the recent paper “Measuring coverage of infant and young child feeding counselling interventions: A framework and empirical considerations for survey question design”. Sunny helped me unpack IYCF coverage and the benefits of the measurement framework she and her co-authors propose.

©2010 SPRING, Courtesy of USAID/SPRING-UNICEF IYCF Digital Image Bank
Q: What is IYCF counselling and support? What are IYCF practices? What is coverage?
“Infant and young child feeding (IYCF)” focuses on the nutritional needs and feeding practices in children under two years of age, which includes both adequate breastfeeding and complementary feeding practices.
“Counseling” is often difficult to translate, and some languages use the same word as “advising.” Technically speaking, counseling is more than advising, which refers to telling people what you think they should do. When you counsel, you listen and try to understand how people feel, then help every person decide which options or suggestions are best for them and help them to have the confidence to carry out their decisions. However, from the perspective of clients or beneficiaries receiving counseling, she/he is unlikely to recognize or understand this distinction, so we end up simplifying it to whether a service provider has “talked with you about…”. Thus, the responsibility is on the service providers to provide “counseling”, and the clients or beneficiaries may simply recall the interaction having taken place. “IYCF counseling and support” includes any other assistance or “support” from service providers and/or peers to build confidence and skills/abilities for breastfeeding and complementary feeding.
“IYCF practices” are the applications or actions of mothers and caregivers in appropriately feeding children under two years of age; these include early initiation of breastfeeding within one hour of birth, exclusive breastfeeding for the first six months of life, and introduction of nutritionally-adequate and safe complementary foods at six months together with continued breastfeeding up to two years of age or beyond.
“Coverage” is the proportion of individuals who need a service or intervention who actually receive it. So, for IYCF counseling coverage, the indicator is the proportion of mothers/caregivers with children under two years of age who received IYCF counseling.
Q: Why is it important to measure both IYCF practices, and counseling and support?
As a behavioral outcome for good child nutrition, it is important to measure whether mothers/caregivers are doing these recommended practices, but from the side of service delivery, it is also necessary to measure whether the services or interventions to support practices are being provided. One is not a good proxy measure for the other.
Q: What have we learned about measuring IYCF counseling so far and what makes measuring coverage of IYCF counselling challenging?
When developing a survey question to measure coverage, we have to ask about the service or intervention in the way that clients/beneficiaries recognize and understand it, and we have to ask about receipt of that service or intervention within a specified period of time. In the case of IYCF counseling, both issues are complicated by the complexity of IYCF counseling interventions. That is, IYCF counseling involves a variety of different age-specific topics and messages (e.g. about breastfeeding and/or complementary feeding); it may be provided in various locations (e.g. at a health facility, at home, or another place else in the community); it may be provided by various service providers (e.g. nurses, midwives, community health agents, NGO workers, skilled counselors, etc.); it may be provided frequently or highly infrequently, briefly or at length; it may be provided in person or by mobile phone. These may vary by country, region and context. Additionally, it must be distinguished from advice or messages provided by unskilled providers such as family, friends and neighbors, or from infant formula advertisements.
Q: The paper proposes a framework for 6-elements for measuring IYCF counseling in household surveys. Do you think this framework is appropriate for all settings?
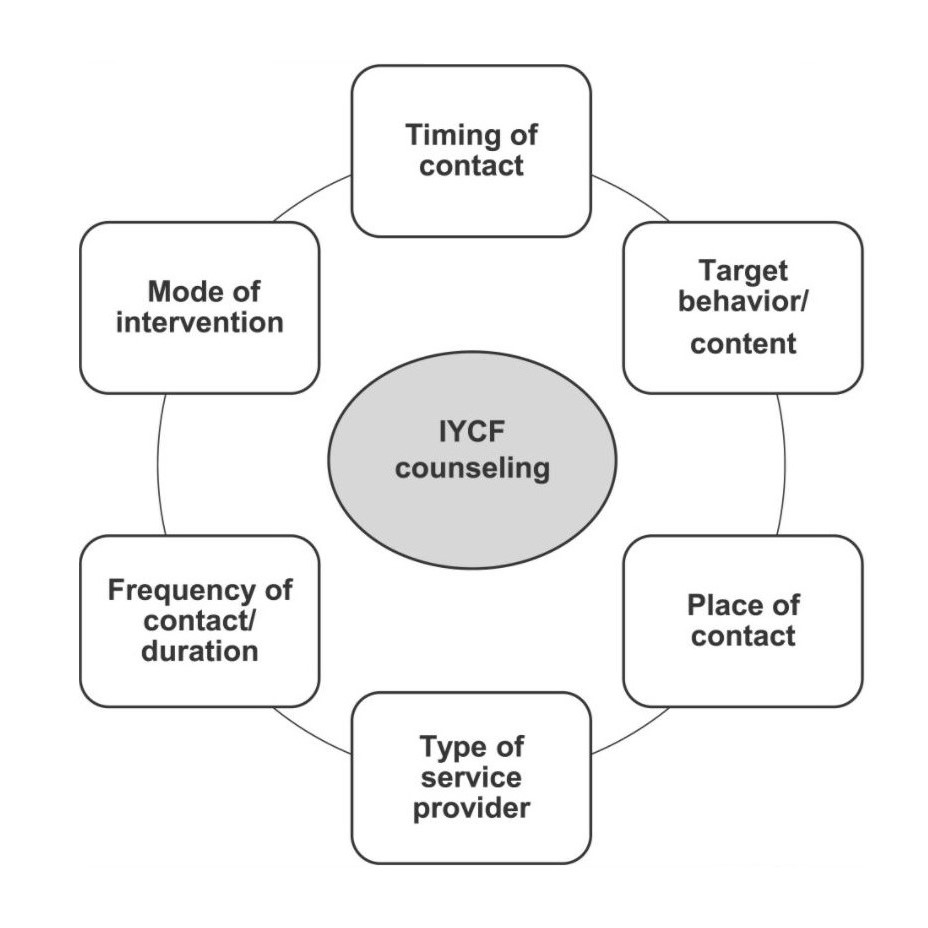
Choufani et al (2020) Figure 1: Six elements of IYCF counselling coverage questions. IYCF, infant and young child feeding
’No’ in direct application, but ‘yes’ in consideration. It is important to consider the purpose and context of the household survey. It may not be feasible or necessary to administer multiple questions to capture details about all elements. However, all elements should be considered when developing or adapting even a single question about IYCF counseling coverage.
For instance, for a large-scale nationally representative household survey covering a lot of different topics and questions, such as the Demographic and Health Surveys (DHS), you might include a single overall question about IYCF counseling coverage. Still, one should consider what types of service providers generally provide IYCF counseling in that country, so that the survey question may be specified to “health care provider and community health agents” if those cadres are key providers.
In the case of household surveys for program evaluation where IYCF counseling is an intervention, it may be feasible and of interest to administer questions to capture all elements.
Q: The paper cites several challenges to measuring IYCF counseling—including recall, prompted vs. unprompted, and validity. What benefits do you see in applying the framework to account for those challenges?
We often overlook or underestimate at best the effort required for and the effects of developing good survey questions. Considering how to minimize recall bias, making a trade-off between a prompted question (easier to administer) and an unprompted or open-ended question (may reduce response error), and testing the validity of a question and response accuracy should be part of good practices of researchers who apply household surveys. The benefits will be reaped in better survey administration, less confused or frustrated respondents, and more accurate responses or higher quality data.
Q: What kind of feedback have you received about the paper so far?
After the paper was published in April, this work was presented at the Global Breastfeeding Collective meeting in May. Among the co-authors, we have members of WHO/UNICEF Technical expert advisory group on nutrition Monitoring (TEAM), so we believe it will be applicable to their work.
This work is building towards the next stages for empirically testing coverage questions. Some IYCF counseling coverage questions have been added to the DHS-8 (2018-2023). Cognitive interviewing has been conducted around these new questions and, as part of joint work by Improve (formerly Improving Coverage Measurement for MNCH) and DataDENT, there is a plan to conduct validation studies in India and Nepal.
In March 2020, UNICEF, the Global Nutrition Cluster, and the Global Technical Assistance Mechanism for Nutrition issued the joint guidance “Infant and Young Child Feeding in the Context of COVID-19”. This guidance highlights IYCF counseling and support to pregnant women and mothers/caregivers with infants and young children as critical services in the context of COVID-19. In order to ensure services are being received, it is crucial that we measure coverage of these interventions.